The structure and basic principles of optical coherence tomography.
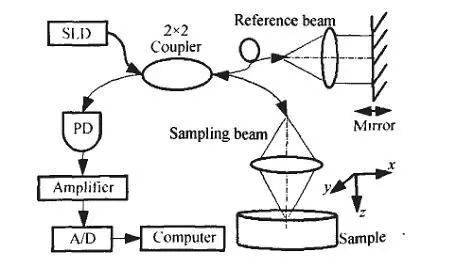
Optical coherence tomography is based on the principle of interferometer, uses near-infrared weak coherent light to irradiate the tissue to be tested, and generates interference based on the coherence of the light. It uses superheterodyne detection technology to measure the intensity of reflected light for superficial tissue imaging. . The OCT system is composed of a low-coherence light source, a fiber-optic Michelson interferometer, and a photoelectric detection system.
The core of OCT is the fiber Michelson interferometer. The light emitted by the low-coherence light source Superluminescence Diode (SLD) is coupled into the single-mode fiber, and is divided into two paths by the 2×2 fiber coupler. One way is the reference light that is collimated by the lens and returned from the plane mirror. ; The other is the sampling beam focused by the lens to the sample under test.
The reference light returned by the reflector and the backscattered light of the sample under test merge on the detector. When the optical path difference between the two is within the coherence length of the light source, interference occurs. The output signal of the detector reflects the backscatter of the medium. Toward scattering intensity.
Scan the mirror and record its spatial position, so that the reference light interferes with the backscattered light from different depths in the medium. According to the mirror position and the corresponding interference signal intensity, the measurement data of different depths (z direction) of the sample is obtained. Then combined with the scanning of the sampling beam in the x-y plane, the result is processed by the computer to obtain the three-dimensional structure information of the sample.
The development of OCT imaging technology
With the widespread application of ultrasound in the field of ophthalmology, people hope to develop a higher resolution detection method. The emergence of Ultrasound Biomicroscope (UBM) meets this requirement to a certain extent. It can perform high-resolution imaging of the anterior segment by using higher frequency sound waves. However, due to the rapid attenuation of high-frequency sound waves in biological tissues, its detection depth is limited to a certain extent. If light waves are used instead of sound waves, can the defects be compensated?
In 1987, Takada et al. developed an optical low-coherence interferometry method, which was developed into a method for high-resolution optical measurement with the support of fiber optics and optoelectronic components; Youngquist et al. developed an optical coherent reflectometer whose light source is A super light-emitting diode directly coupled to an optical fiber. One arm of the instrument containing a reference mirror is located inside, while the optical fiber in the other arm is connected to a camera-like device. These have laid the theoretical and technical basis for the emergence of OCT.
In 1991, David Huang, a Chinese scientist at MIT, used the developed OCT to measure the isolated retina and coronary arteries. Because OCT has unprecedented high resolution, similar to optical biopsy, it was quickly developed for the measurement and imaging of biological tissues.
Due to the optical characteristics of the eye, OCT technology is developing fastest in ophthalmology clinical applications. Before 1995, scientists such as Huang used OCT to measure and image tissues such as the retina, cornea, anterior chamber and iris of the in vitro and in vivo human eyes, continuously improving OCT technology. After several years of improvement, the OCT system has been further improved and developed into a clinically practical detection tool, made into a commercial instrument, and finally confirmed its superiority in fundus and retinal imaging. OCT was officially used in ophthalmology clinics in 1995.
In 1997, OCT was gradually used in dermatology, digestive tract, urinary system and cardiovascular examinations. Esophagus, gastrointestinal, urinary system OCT and cardiovascular OCT are all invasive examinations, similar to endoscopes and catheters, but with higher resolution and can observe ultrastructures. Skin OCT is a contact inspection, and ultrastructure can also be observed.
The initial OCT used in clinical practice is OCT1, which is composed of a console and a power console. The console includes an OCT computer, an OCT monitor, a control panel and a monitoring screen; the power station includes a fundus observation system and an interference light control system. Since the console and the power platform are relatively independent devices, and the two are connected by wires, the instrument has a larger volume and a larger space.
The analysis program of OCT1 is divided into image processing and image measurement. Image processing includes image standardization, image calibration, image calibration and standardization, image Gaussian smoothing, image median smoothing; image measurement procedures are less, only retinal thickness measurement and retinal nerve fiber layer thickness measurement. However, because OCT1 has fewer scanning procedures and analysis procedures, it was quickly replaced by OCT2.
OCT2 is formed by software upgrade on the basis of OCT1. There are also some instruments that combine the console and the power table into one to form an OCT2 instrument. This instrument reduces the image monitor and observes the OCT image and monitors the patient's scanning position on the same computer screen, but the operation is the same as OCT1 Similar, it is manually operated on the control panel.
The appearance of OCT3 in 2002 marked a new stage of OCT technology. In addition to the more user-friendly operation interface of OCT3, all operations can be done on the computer with the mouse, and its scanning and analysis programs are becoming more and more perfect. More importantly, the resolution of OCT3 is higher, its axial resolution is ≤10 μm, and its lateral resolution is 20 μm. The number of axial samples acquired by OCT3 has increased from 128 to 768 in the original 1 A-scan. Therefore, the integral of OCT3 has increased from 131 072 to 786 432, and the hierarchical structure of the scanned tissue cross-sectional image is clearer.
Copyright @ 2020 Shenzhen Box Optronics Technology Co., Ltd. - China Fiber Optic Modules, Fiber Coupled Lasers Manufacturers, Laser Components Suppliers All Rights Reserved.